cpr in pregnancy

Cardiac arrest in pregnancy is rare, occurring in approximately one in 30,000 pregnancies (Hill, 2009). Despite pregnant women being younger than the traditional cardiac arrest patient, the survival rates are poorer, with one case series reporting a survival rate of 6.9% (Vanden Hoek et al., 2010) Initiation of CPR should be prompt while addressing the cause of the arrest. The standard ACLS algorithms should be applied for medications, intubation, and defibrillation. Chest compressions and ventilations should also be performed according to American Heart Association guidelines with the understanding that they are less effective in the latter part of the pregnancy due to compromised cardiac output from aortocaval compression.
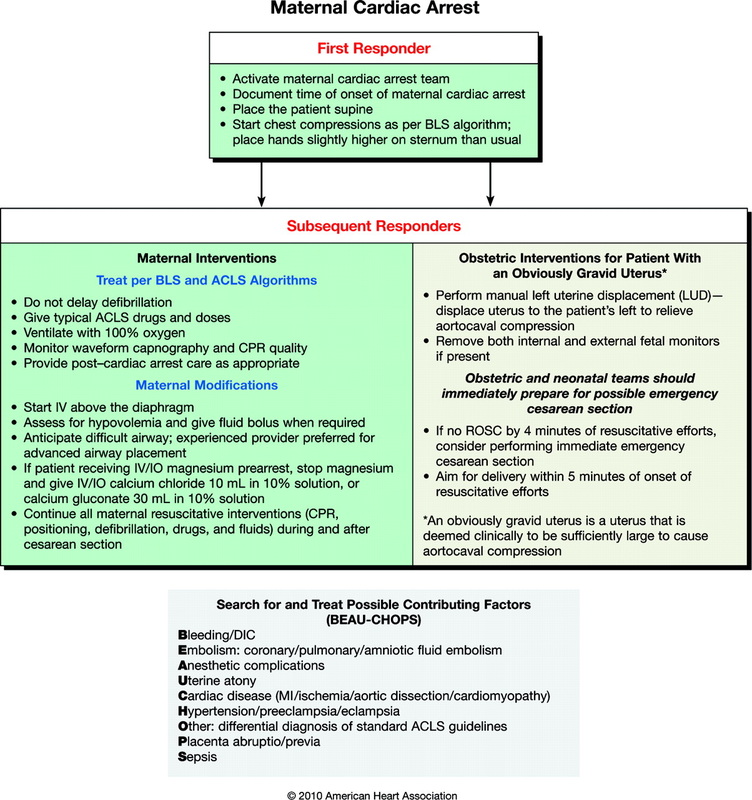
During the attempted resuscitation, providers must recognize that they have two potential patients: the mother and the fetus. The best hope of fetal survival is the survival of the mother (Vanden Hoek, 2010). The following guidelines are from the 2010 AHA Guidelines for Cardiac Arrest in special situations and are the standard of care for treating critically ill pregnant patients.
1. Place the patient in full left lateral position to relieve possible compression of the inferior vena cava.
Uterine obstruction of venous return can produce hypotension and may precipitate arrest. If the left lateral
decubitus position cannot be achieved, manual displacement of the uterus to the left may be performed.
Patient position has emerged as an important strategy to improve the quality of CPR and resultant
compression force and output. Reports of non-cardiac arrest patients indicate that the left-lateral tilt position
results in improved maternal hemodynamics of blood pressure, cardiac output and stroke volume, and
improved fetal parameters of oxygenation, nonstress test and fetal heart rate. Two studies of pregnant
women not in arrest found that manual left uterine displacement, which is done with the patient supine,
is as good or better than left-lateral tilt in relieving aortocaval compression (Vanden Hoek et al, 2010).
Chest compressions should be placed slightly higher on the sternum to adjust for elevation of the diaphragm
and abdominal contents caused by the gravid uterus.
2. Give 100% high flow oxygen
3. Establish intravenous (IV) access above the diaphragm.
4. Assess for hypotension. Maternal hypotension that warrants therapy has been defined as a systolic blood
pressure <100 mm Hg or < 80% of baseline. Maternal hypotension can result in reduced placental perfusion.
5. Consider reversible causes of critical illness and treat conditions that may contribute to clinical deterioration
as early as possible.
6. If there is no return of spontaneous circulation (ROSC) within 4 minutes of resuscitative efforts, an emergency
cesarean section should be performed, with the goal of delivery within 5 minutes.
During the attempted resuscitation, providers must recognize that they have two potential patients: the mother and the fetus. The best hope of fetal survival is the survival of the mother (Vanden Hoek, 2010). The following guidelines are from the 2010 AHA Guidelines for Cardiac Arrest in special situations and are the standard of care for treating critically ill pregnant patients.
1. Place the patient in full left lateral position to relieve possible compression of the inferior vena cava.
Uterine obstruction of venous return can produce hypotension and may precipitate arrest. If the left lateral
decubitus position cannot be achieved, manual displacement of the uterus to the left may be performed.
Patient position has emerged as an important strategy to improve the quality of CPR and resultant
compression force and output. Reports of non-cardiac arrest patients indicate that the left-lateral tilt position
results in improved maternal hemodynamics of blood pressure, cardiac output and stroke volume, and
improved fetal parameters of oxygenation, nonstress test and fetal heart rate. Two studies of pregnant
women not in arrest found that manual left uterine displacement, which is done with the patient supine,
is as good or better than left-lateral tilt in relieving aortocaval compression (Vanden Hoek et al, 2010).
Chest compressions should be placed slightly higher on the sternum to adjust for elevation of the diaphragm
and abdominal contents caused by the gravid uterus.
2. Give 100% high flow oxygen
3. Establish intravenous (IV) access above the diaphragm.
4. Assess for hypotension. Maternal hypotension that warrants therapy has been defined as a systolic blood
pressure <100 mm Hg or < 80% of baseline. Maternal hypotension can result in reduced placental perfusion.
5. Consider reversible causes of critical illness and treat conditions that may contribute to clinical deterioration
as early as possible.
6. If there is no return of spontaneous circulation (ROSC) within 4 minutes of resuscitative efforts, an emergency
cesarean section should be performed, with the goal of delivery within 5 minutes.